
2·
1 day agoAs a medical student with an absurd amount of student loans, this stuff is very important to me.
As a medical student with an absurd amount of student loans, this stuff is very important to me.
No, that was applicable to anyone enrolled in the SAVE plan. If you made more money than that, you would have a small payment which was limited to 5% of your discretionary income (a number that excludes a portion of your income as non-discretionary for living expenses, etc). So if you made 75k/year, your payment would be 5% of the amount not designated as necessary living expenses. I’m not positive on the exact numbers, but I think they exclude about 60k before they start calculating your payment amount.
That’s basically what the SAVE plan did. If you enrolled in it and made qualifying income-based payments that didn’t cover the interest on the loan, the interest wouldn’t capitalize and it would still count as a qualifying payment for PSLF. It wasn’t loan forgiveness, but it ensured that payers wouldn’t have their loan balances skyrocket while making income-driven repayments.

Unfortunately, most health insurance plans have a separate sub-company manage the pharmacy benefits and we have absolutely zero way of accessing their systems. It would be lovely if we could see what your insurance would cover immediately as we prescribe it, but that also runs into the problem of us not having any control over the actual pharmacy and their billing and pricing.

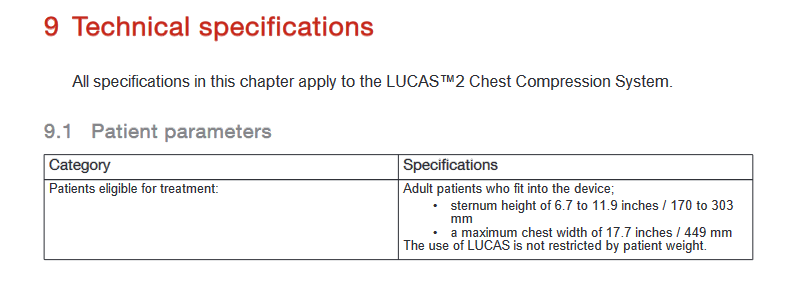
And as long as CPR machines are obscenely expensive and difficult to obtain and maintain for a lot of smaller hospitals and EMS systems.
Here’s the problem with that: it relies on things like the LUCAS CPR assist machine which doesn’t fit on a lot of people. I’ve done CPR on a lot of people, and only a handful of them would have even fit in a LUCAS in the first place.
In this case, it’s the medical ethics standards that have been discussed, litigated, and debated to hell and back before landing on the accepted standard. So it’s the physicians, lawyers, ethics experts, legislators, and judicial system that agreed on what is best.
The issue is that we do provide education and try to have these conversations, but the information is also available in layman’s terms from reputable organizations like the CDC. It all falls on deaf ears though. There is no evidence that shows any benefit for a delayed vaccination schedule with just a tiny number of exceptions for rare immune disorders. The other part of it is that it can become a burden on the clinic to deal with a bunch of extra appointments and having to fill out all the paperwork for the school/daycare explaining why the under/un-immunized child should be allowed in school anyways…and when you see 20 patients a day in the office and have another couple dozen phone calls, messages, and consults to deal with every day as well, spending the time to convince someone to accept scientific consensus in the place of the facebook posts they read is a tall order.
Yes. This exactly.
The problem with the “delayed” vaccination schedule is that then you get un- or under-immunized babies in daycare because the maternity/paternity leave runs out and the kid has to go to daycare. The way the vaccination schedules are currently implemented are done so to provide the best protection for the child on a timeline that would match up with the physiologic development of their immune system, the loss of immunoglobulin transfer from breast milk, and the exposure to more pathogens in environments outside the home.
Medical professional giving my two cents here: physicians and healthcare providers are allowed, and in some cases even required, to disregard the expressed, voiced, or even written wishes of the parent if the parent’s wishes would endanger the child’s life. The classic example is with Jehovah’s Witnesses: if a child of a Jehovah’s Witness is getting surgery or suffered an injury with significant blood loss, the child will be given life-saving blood transfusions irrespective of the parents’ religious beliefs or wishes.
This is not a breach of informed consent taken lightly, but physicians and other medical professionals will ignore what the parents did or did not consent to if it means that the child or vulnerable adult would die or suffer grievous harm otherwise.
I’m in my third year of medical school, so I’ve just started my clinical rotations, but one of the things that shows up on almost every reference table for physicians regarding treatment options is information on the price for the patient. I’m rotating in a family medicine clinic right now, and we pretty frequently prescribe the best possible treatment, and then when the pharmacy runs it through the patient’s insurance and finds out how much it’s going to cost, we then start working down the list of next-best alternatives until we can find something the patient can afford. Because there are so many different insurance plans out there, we have no idea how much something is going to cost until the insurance tells us.
Medical field here: The vast majority of us are not in it for the money. Physicians have to spend 3 to 9 years after medical school working for a wage that works out to about $5/hour to gain certification and a medical license in their specialty. And that’s after 8 to 12 years of undergraduate/graduate/doctorate education that basically has to be paid for with loans unless they’re in the military or come from a rich family. So, yes, physicians do make high salaries once they’re established, but there was a lot of work and sacrifice to get to that point, and very few people are masochistic enough to put themselves through that just for the money.
Also, the most expensive parts of a medical appointment/surgery/ER visit etc is the administrative overhead, inflated prices of drugs and supplies, and insurance company bullshit. Very little money from that price tag actually makes it to the healthcare workers. Your average EMT on an ambulance makes between $13-20/hour depending on the state minimum wage.
If you have a problem with your healthcare costs, that’s something to take up with your representatives in government, not the EMTs, CNAs, nurses, and physicians providing your care.
I think the bigger issue is the lack of scholarships for non-athletic activities. There are many other things that colleges and universities could give scholarships for that would foster a more diverse and inclusive student body, but the preferential treatment given to athletes actually impedes that through diversion of funds.
I was rather happy when my alma mater decided to use a pile of alumni association money to build a massive LAN center and start pro e-sports teams instead of starting a football program. The e-sports program will give scholarships not just for the gamers, but also for theater kids that become shoutcaster personalities, and they use the LAN center as a way to beta test the games coming out of the game development programs. They really emphasize the educational aspect of it as well and push the gamers to get involved in game design or creative writing majors/minors so that their scholarship activity can actually benefit their career after school. It does help that the school is down the road from Acti-Blizz, so internships are plentiful.
There are other ways for the schools to support potentially profitable student activities that don’t exclude people unable to participate in sports.
Mayo, Stanford, University of Michigan and University of Minnesota all turn out more research than Harvard does, and those are just the tip of the iceberg. Harvard is a big name, but they aren’t making the big breakthroughs anymore.
Also the ivy league medical schools don’t provide as much in the way of community medical services as the others do. To my knowledge, Harvard isn’t out there running critical access hospitals in rural communities at a loss like Mayo and University of Minnesota are.
(And I’m absolutely positive that there are a bunch of other state universities and medical programs that do just as much as Mayo and University of Minnesota in terms of community medical services, but I’m just not as familiar with them )
It completely excludes a lot of people with physical disabilities or health problems though. I promise you that the kid with a chronic health condition that has them in and out of the hospital while they’re getting through school is a harder worker than the captain of the football team that’s just maintaining their GPA to stay on the team.
Edit: Also, it’s sexist as hell. The best scholarships are for men’s sports and many women’s sports don’t get anywhere near the same support as men’s sports, even in equivalent ones like soccer and basketball. There’s no women’s football league, and the women’s leagues for other sports are abysmally supported.
That’s the idea.

The PE bullshit is why I want to be a physician in the public, county ER that actually employs its physicians directly. Also, the PE companies don’t qualify for PSLF, and they don’t pay enough to make up that difference against non-profit hospitals.

That’s part of my point. My American education was pretty limited on the internal politics and civics of other countries, but my husband who went to high school in a different state did get a decent amount of information about how modern/current European countries are structured. So I guess it’s safe to assume that other countries will also have differences across regions.

It’s variable, but some people have one where the upper lip connects to the gums and another one for the bottom lip. So an AMAB can have up to 4 of them.